

Gastric Sleeve Surgery (Vertical Sleeve Gastrectomy)
Medically Reviewed by: Dr. Vytauras Kuzinkovas
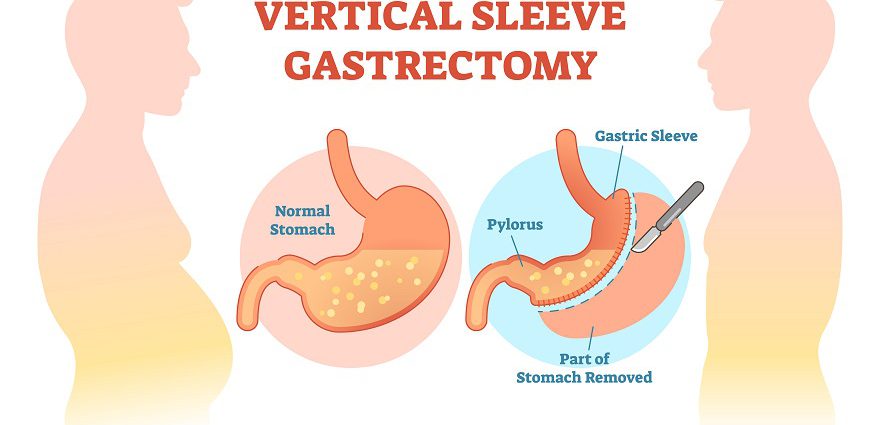
Gastric sleeve surgery, or vertical sleeve gastrectomy, is one of the newer types of bariatric surgery. It can also be referred to medically as gastric sleeve resection, sleeve gastrectomy, tube gastrectomy or laparoscopic sleeve gastrectomy.
How it Works
During this procedure a bariatric surgeon removes about 85 percent of the stomach so that it takes the shape of a tube or sleeve. This operation is performed laparoscopically, meaning that the surgeon makes small incisions as opposed to one large incision. He or she inserts a viewing tube with a small camera (laparoscope) and other tiny instruments into these small incisions to remove part of the stomach. The tube-shaped stomach that is left is sealed closed with staples.
In some cases, gastric sleeve surgery may be followed by a gastric bypass surgery or duodenal switch surgery after a person has lost a significant amount of weight. Called a “staged” approach to weight loss surgery, this makes the second procedure less risky than it would have been had it been the first and only procedure. The timing of the second surgery varies according to the degree of weight loss. It usually occurs within six to 18 months after the initial surgery.
Who Is a Good Candidate?
No reliable statistics exist yet for how many of these procedures have been done. The current scientific literature supports use of sleeve gastrectomy as a primary bariatric procedure. This means that the indications for the sleeve are the same as other covered procedures such as gastric bypass or adjustable gastric banding. The National Institutes of Health (NIH) requires a body mass index (BMI) greater than 40. This is the equivalent of being about 100 pounds overweight for men and 80 pounds overweight for women. People with BMIs between 35 and 39 may also be candidates for weight loss surgery if they have obesity-related illnesses such as diabetes, high blood pressure or high cholesterol. A BMI takes height and weight into account to measure body fatness. A BMI of 30 or higher in adults is considered obese.
(Read more about body mass index, and use our BMI calculator.)
Gastric sleeve surgery also may be appropriate for people who can’t return as often for the follow-up visits required by gastric banding procedures such as Lap Band surgery or Realize Band surgery.
What to Do Before Surgery
Before gastric sleeve resection or any bariatric surgery, you must quit smoking, as smoking increases the risk for infections, pneumonia, blood clots, slow healing and other life-threatening complications after surgery. Ideally, you should permanently quit smoking, but even if you don’t you must quit for at least one month before and one month after bariatric surgery.
Some surgeons require patients to go on special diets in the week(s) before the procedure.
What to Expect After Surgery
A non-reversible procedure, gastric sleeve surgery is performed under general anesthesia and takes about one to two hours. Afterward you will probably stay in the hospital for one or two days; recovery may last a few weeks.
The abdomen is often swollen and sore for several days. Your surgeon may prescribe pain medication for the discomfort. Some scarring may occur, but this can be covered with clothing.
Following surgery, you will need to become re-accustomed to eating solid foods. Normally this starts with two weeks on a liquid-only diet, two weeks of semi-solid, pureed foods and then solids.
As far as weight loss goes, most people who have gastric sleeve surgery lose 50 to 80 percent of their excess body weight over the first six months to one year after surgery. Studies have shown that after the gastric sleeve resection procedure people show improvement in diabetes, high blood pressure, high cholesterol and sleep apnea within one to two years. These improvements are comparable with those seen after other weight loss surgeries.
As this is a relatively new procedure, limited data is available on long-term weight loss (beyond five years after surgery) or overall health improvements.
Following recovery, certain lifestyle changes and follow-up care occur; people who have gastric sleeve surgery must:
- Exercise regularly.
- Learn behavior modification techniques.
- Follow very specific dietary instructions for the rest of their lives, including eating very slowly, consuming only small quantities of food at a time, chewing thoroughly and swallowing food only when it is mashed, and not eating and drinking at the same time.
(Read more about gastric sleeve recovery.)
Risks and Complications
There are several risks and complications of gastric sleeve surgery:
- Leaking of the sleeve. The operation requires stapling inside the stomach, and there is always a chance that the staples won’t hold, resulting in a leak. The leaking stomach acids frequently lead to infection of surrounding tissues and other serious problems that may require another operation or a drainage tube.
- Blood clots
- Weight may be regained over time, because the stomach can stretch.
Since this procedure is relatively new, long-term risks and benefits are not known. However, it does have several advantages over gastric banding and other surgical procedures. For example:
- Wound infection
- Unlike gastric banding surgeries, no foreign objects are left in the body during the procedure. With gastric banding, the band may slip, erode or become infected.
- Unlike gastric bypass or duodenal switch, there is no bypass of the small intestines with the gastric sleeve, so all nutrients are absorbed and very little chance exists of absorption issues.
(Read more about the risks of gastric sleeve surgery.)
Cost of Gastric Sleeve Surgery
While this procedure is relatively new, insurers are beginning to cover the cost of gastric sleeve surgery; among those doing so are Aetna, Cigna, HCSC, and United Healthcare. The cost of gastric sleeve surgery can exceed $10,000.
(Read more about the cost of gastric sleeve surgery.)
Plastic Surgery After Massive Weight Loss
Although the full extent of weight loss may not occur until after a second procedure has been performed, such as gastric bypass, it is important to know that plastic surgery after massive weight loss may be necessary to remove excess skin and fat and create a more shapely body profile. Arm lift surgery and body lift are common post-bariatric procedures.
About the Reviewer
 Vytauras Kuzinkovas, MBBS, MD, MRCSEd, FRCSEd, FRACS, is a fellowship-trained, board-certified general / upper gastrointestinal surgeon treating bariatric surgery patients at Advanced Surgicare clinic, his state-of-the-art Sydney bariatric clinic in New South Wales, Australia. Dr. Kuzinkovas has performed more than 5,000 laparoscopic surgeries as well as countless endoscopic procedures. He completed a postgraduate research fellowship in laparoscopic surgery and surgical immunology under the tutelage of Professor Markus Büchler, an internationally renowned upper-gastrointestinal and pancreatic surgery specialist. Dr. Kuzinkovas is a Fellow of the Royal Australasian College of Surgeons (FRACS), the Royal College of Surgeons of Edinburgh (FRCSEd) and the Royal Society of Medicine of Britain. Learn More
Vytauras Kuzinkovas, MBBS, MD, MRCSEd, FRCSEd, FRACS, is a fellowship-trained, board-certified general / upper gastrointestinal surgeon treating bariatric surgery patients at Advanced Surgicare clinic, his state-of-the-art Sydney bariatric clinic in New South Wales, Australia. Dr. Kuzinkovas has performed more than 5,000 laparoscopic surgeries as well as countless endoscopic procedures. He completed a postgraduate research fellowship in laparoscopic surgery and surgical immunology under the tutelage of Professor Markus Büchler, an internationally renowned upper-gastrointestinal and pancreatic surgery specialist. Dr. Kuzinkovas is a Fellow of the Royal Australasian College of Surgeons (FRACS), the Royal College of Surgeons of Edinburgh (FRCSEd) and the Royal Society of Medicine of Britain. Learn More